Mindfulness for Mental Health: Discover the Benefits of Guided Meditation and Relaxation Techniques-Let’s face it: mental health is a huge part of our overall well-being. But many of us grapple with anxiety and stress on a daily basis. If that sounds familiar, you’re not alone! One effective way to tackle those feelings is through mindfulness practices like guided meditation and relaxation techniques. In this friendly guide, we’ll dive into how tools like […]
The Essential Health Benefits of Regular Physical Activity: A Guide to Thriving Through Movement-Introduction Hey there! Have you ever considered how something as simple as a daily walk could help lower your chances of serious health issues? It’s pretty amazing, right? Engaging in regular physical activity can do wonders for both your body and mind. When we weave movement into our daily lives, we open the door to a whole bunch of benefits—from […]
How Your Diet Affects Sleep Quality: Eat for Restful Nights-Let’s face it—sleep matters. It’s not just about closing your eyes and hoping for the best; sleep is a crucial player in how we feel, think, and live our lives. Did you know that what you eat plays a big role in determining how well you sleep? It’s true! While sleep quality can be impacted by various factors, research shows […]
Daily Workouts – Home Fitness: Your Ultimate Guide to Effective At-Home Exercise-Staying fit shouldn’t come with the stress of a gym membership or having to buy a ton of fancy equipment that takes over your living room. Enter the Daily Workouts – Home Fitness app by Daily Workout Apps, LLC. It’s packed with quick and effective workouts that everyone, no matter their fitness level, can jump into. In this guide, we’re […]
Discovering the Benefits of Mindfulness: How Headspace Can Help You Feel Better-Ever feel like stress and anxiety are clinging to you as constant companions? You’re not alone. In a world that moves at breakneck speed, many of us are searching for ways to take charge of our mental health. That’s where Headspace comes in. This meditation app, created by Andy Puddicombe, offers an easy way to weave mindfulness into your daily […]
How Regular Physical Activity Boosts Your Cardiovascular Health-Hey there! Let’s talk about something really important: keeping your heart healthy in today’s world, where it’s all too easy to get caught up in a sedentary lifestyle. Ever wonder how something as simple as moving your body more can lead to better cardiovascular health? You’re in the right spot! The truth is, whether you’re squeezing in more steps during […]
Mastering Anxiety Management: Practical Strategies Backed by Expert Insights-Anxiety can feel like a heavy weight on your chest, especially when it sneaks up during a hectic workday or crashes down on a quiet evening. If you’ve ever found yourself grappling with these feelings, you’re not alone. Understanding how to manage anxiety is essential for reclaiming your peace of mind. In this guide, we’ll dive into practical strategies recommended […]
Understanding Anxiety Management: Insights from Dr. Bethany Juby-Anxiety is something many of us face. It can creep into our daily lives, bringing along physical discomfort, mental hurdles, and emotional pain. But here’s the good news: with the right strategies, we can manage anxiety and significantly boost our overall well-being. Dr. Bethany Juby, a licensed clinical psychologist who specializes in trauma recovery and stress management, shares her valuable […]
The Ultimate Guide to Effective At-Home Workouts: Body Weight Exercises for Every Level-Staying fit without making a trip to the gym might sound like a stretch, but it’s totally doable—even if you’re tight on time or feeling less than motivated. In today’s busy world, at-home workouts using body-weight exercises have gained traction among fitness fans, whether they’re just starting out or already buff. In this guide, we’ll dive into why at-home workouts […]
Your Ultimate Guide to Heart Health: The Benefits of Staying Active-Staying active isn’t just about hitting the gym; it’s about making a commitment to your health and happiness every day. If you want to boost your heart health and improve your overall quality of life, then weaving regular physical activity into your routine is non-negotiable. Let’s dive into how moving your body can drastically enhance your physical and mental well-being, […]
 Mindfulness for Mental Health: Discover the Benefits of Guided Meditation and Relaxation Techniques - Let’s face it: mental health is a huge part of our overall well-being. But many of us grapple with anxiety and stress on a daily basis. If that sounds familiar, you’re not alone! One effective way to tackle those feelings is through mindfulness practices like guided meditation and relaxation techniques. In this friendly guide, we’ll dive into how tools like […]
Mindfulness for Mental Health: Discover the Benefits of Guided Meditation and Relaxation Techniques - Let’s face it: mental health is a huge part of our overall well-being. But many of us grapple with anxiety and stress on a daily basis. If that sounds familiar, you’re not alone! One effective way to tackle those feelings is through mindfulness practices like guided meditation and relaxation techniques. In this friendly guide, we’ll dive into how tools like […] The Essential Health Benefits of Regular Physical Activity: A Guide to Thriving Through Movement - Introduction Hey there! Have you ever considered how something as simple as a daily walk could help lower your chances of serious health issues? It’s pretty amazing, right? Engaging in regular physical activity can do wonders for both your body and mind. When we weave movement into our daily lives, we open the door to a whole bunch of benefits—from […]
The Essential Health Benefits of Regular Physical Activity: A Guide to Thriving Through Movement - Introduction Hey there! Have you ever considered how something as simple as a daily walk could help lower your chances of serious health issues? It’s pretty amazing, right? Engaging in regular physical activity can do wonders for both your body and mind. When we weave movement into our daily lives, we open the door to a whole bunch of benefits—from […] How Your Diet Affects Sleep Quality: Eat for Restful Nights - Let’s face it—sleep matters. It’s not just about closing your eyes and hoping for the best; sleep is a crucial player in how we feel, think, and live our lives. Did you know that what you eat plays a big role in determining how well you sleep? It’s true! While sleep quality can be impacted by various factors, research shows […]
How Your Diet Affects Sleep Quality: Eat for Restful Nights - Let’s face it—sleep matters. It’s not just about closing your eyes and hoping for the best; sleep is a crucial player in how we feel, think, and live our lives. Did you know that what you eat plays a big role in determining how well you sleep? It’s true! While sleep quality can be impacted by various factors, research shows […] Daily Workouts – Home Fitness: Your Ultimate Guide to Effective At-Home Exercise - Staying fit shouldn’t come with the stress of a gym membership or having to buy a ton of fancy equipment that takes over your living room. Enter the Daily Workouts – Home Fitness app by Daily Workout Apps, LLC. It’s packed with quick and effective workouts that everyone, no matter their fitness level, can jump into. In this guide, we’re […]
Daily Workouts – Home Fitness: Your Ultimate Guide to Effective At-Home Exercise - Staying fit shouldn’t come with the stress of a gym membership or having to buy a ton of fancy equipment that takes over your living room. Enter the Daily Workouts – Home Fitness app by Daily Workout Apps, LLC. It’s packed with quick and effective workouts that everyone, no matter their fitness level, can jump into. In this guide, we’re […] Discovering the Benefits of Mindfulness: How Headspace Can Help You Feel Better - Ever feel like stress and anxiety are clinging to you as constant companions? You’re not alone. In a world that moves at breakneck speed, many of us are searching for ways to take charge of our mental health. That’s where Headspace comes in. This meditation app, created by Andy Puddicombe, offers an easy way to weave mindfulness into your daily […]
Discovering the Benefits of Mindfulness: How Headspace Can Help You Feel Better - Ever feel like stress and anxiety are clinging to you as constant companions? You’re not alone. In a world that moves at breakneck speed, many of us are searching for ways to take charge of our mental health. That’s where Headspace comes in. This meditation app, created by Andy Puddicombe, offers an easy way to weave mindfulness into your daily […] How Regular Physical Activity Boosts Your Cardiovascular Health - Hey there! Let’s talk about something really important: keeping your heart healthy in today’s world, where it’s all too easy to get caught up in a sedentary lifestyle. Ever wonder how something as simple as moving your body more can lead to better cardiovascular health? You’re in the right spot! The truth is, whether you’re squeezing in more steps during […]
How Regular Physical Activity Boosts Your Cardiovascular Health - Hey there! Let’s talk about something really important: keeping your heart healthy in today’s world, where it’s all too easy to get caught up in a sedentary lifestyle. Ever wonder how something as simple as moving your body more can lead to better cardiovascular health? You’re in the right spot! The truth is, whether you’re squeezing in more steps during […] Mastering Anxiety Management: Practical Strategies Backed by Expert Insights - Anxiety can feel like a heavy weight on your chest, especially when it sneaks up during a hectic workday or crashes down on a quiet evening. If you’ve ever found yourself grappling with these feelings, you’re not alone. Understanding how to manage anxiety is essential for reclaiming your peace of mind. In this guide, we’ll dive into practical strategies recommended […]
Mastering Anxiety Management: Practical Strategies Backed by Expert Insights - Anxiety can feel like a heavy weight on your chest, especially when it sneaks up during a hectic workday or crashes down on a quiet evening. If you’ve ever found yourself grappling with these feelings, you’re not alone. Understanding how to manage anxiety is essential for reclaiming your peace of mind. In this guide, we’ll dive into practical strategies recommended […]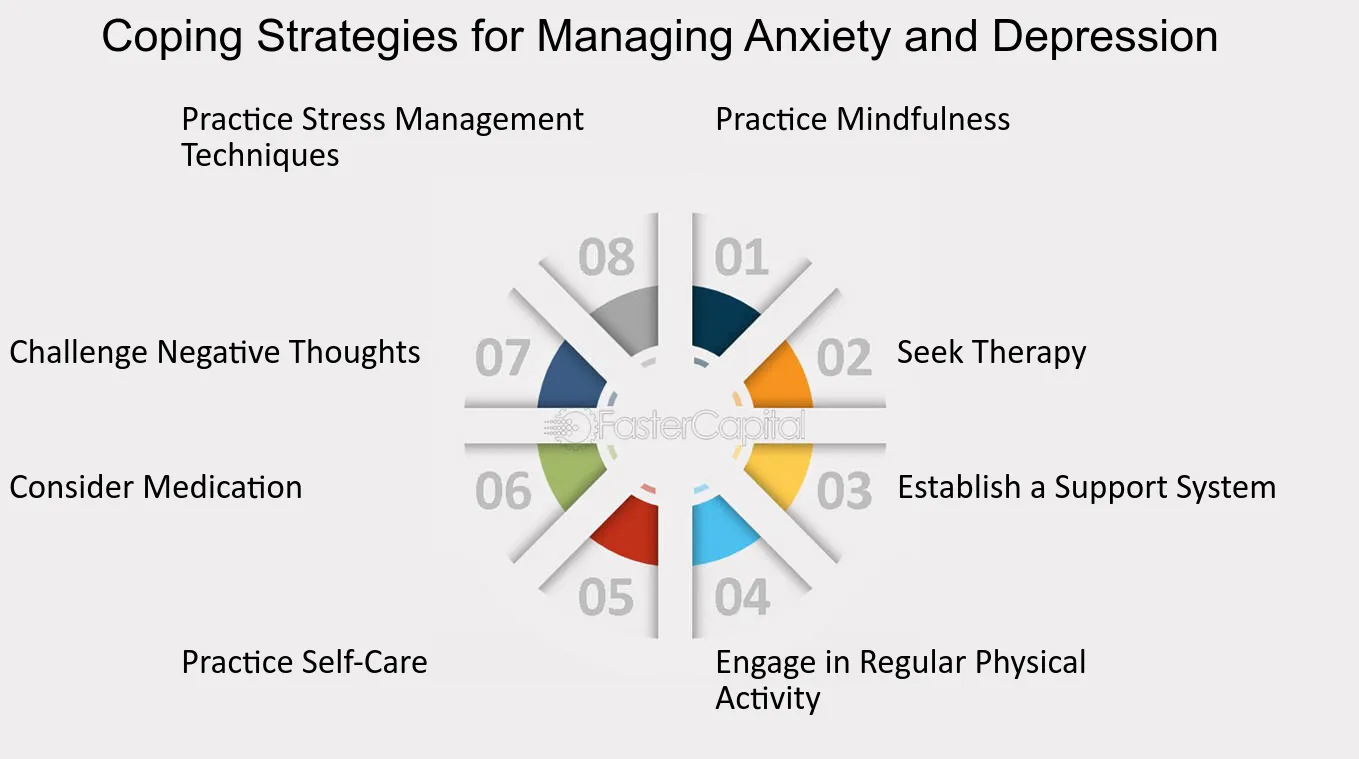 Understanding Anxiety Management: Insights from Dr. Bethany Juby - Anxiety is something many of us face. It can creep into our daily lives, bringing along physical discomfort, mental hurdles, and emotional pain. But here’s the good news: with the right strategies, we can manage anxiety and significantly boost our overall well-being. Dr. Bethany Juby, a licensed clinical psychologist who specializes in trauma recovery and stress management, shares her valuable […]
Understanding Anxiety Management: Insights from Dr. Bethany Juby - Anxiety is something many of us face. It can creep into our daily lives, bringing along physical discomfort, mental hurdles, and emotional pain. But here’s the good news: with the right strategies, we can manage anxiety and significantly boost our overall well-being. Dr. Bethany Juby, a licensed clinical psychologist who specializes in trauma recovery and stress management, shares her valuable […] Your Ultimate Guide to Heart Health: The Benefits of Staying Active - Staying active isn’t just about hitting the gym; it’s about making a commitment to your health and happiness every day. If you want to boost your heart health and improve your overall quality of life, then weaving regular physical activity into your routine is non-negotiable. Let’s dive into how moving your body can drastically enhance your physical and mental well-being, […]
Your Ultimate Guide to Heart Health: The Benefits of Staying Active - Staying active isn’t just about hitting the gym; it’s about making a commitment to your health and happiness every day. If you want to boost your heart health and improve your overall quality of life, then weaving regular physical activity into your routine is non-negotiable. Let’s dive into how moving your body can drastically enhance your physical and mental well-being, […]